Spinal cord tumours
The spine and spinal cord
All the functions and senses of the body are controlled by the central nervous system (CNS). This system is made up of the brain, the spinal cord and a network of peripheral nerves that spread throughout the body from the spinal cord
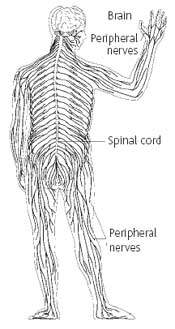
The spinal cord extends from the base of the brain down inside the bones of the backbone, which is also known as the spine or the spinal column. The spinal cord does not extend the full length of the spinal column, but ends in the small of the back (the lumbar area).
Just as the brain is surrounded and protected by the skull, the spinal cord is surrounded and protected by the backbone. The backbone is made up of bones called vertebrae.
There are 26 vertebrae in the spine:
- 7 cervical (neck),
- 12 thoracic (chest area),
- 5 lumbar (lower back),
- the sacrum (pelvic area) and the coccyx (tail bone).
The sacrum and the coccyx are made up of a number of bones that have been joined, or fused together, five in the sacrum and four in the coccyx. The nerves spread out from the spinal cord between the vertebrae.
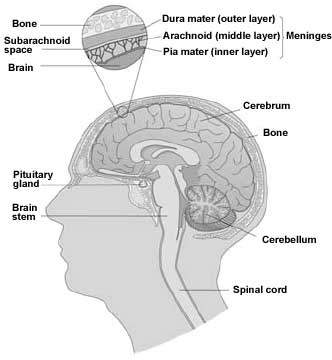
Also surrounding and protecting the brain and spinal cord are the meninges (the membranes that cover the brain and the spinal cord) and a fluid known as cerebrospinal fluid (CSF). There are three different layers making up the meninges; dura mater (outer layer), arachnoid mater (middle) and pia mater (inner).
The spinal cord provides communication between the brain and the rest of the body. Nerve impulses can travel up or down the spinal cord. For example, if we want to pick something up, the brain sends an impulse down the spinal cord and along the nerves that control the functions of the hand. If the object we pick up is soft to touch, an impulse will travel up the spinal cord to the brain to tell us that it has a pleasant feeling. These are known as motor and sensory impulses.
Spinal cord tumours
Cells within the CNS normally grow in an orderly and controlled way, but if for some reason this order is disrupted, the cells continue to divide and form a lump or tumour.
The tumour may be benign, where the cells do not spread from the original site, or malignant (cancerous), where the cells invade and destroy surrounding tissue and may spread to other parts of the CNS.
Tumours affecting the CNS are fairly rare. Just over 5000 new tumours are diagnosed each year in the UK. Many of these are malignant.
Spinal cord tumours can be benign (not cancerous) or malignant (cancerous). Most spinal tumours are benign.
Intramedullary tumours are located within the nerves of the spinal cord. There are several different types of cancer of the spinal cord but the most common are astrocytomas and ependymomas.
Intradural extramedullary tumours start inside the coverings of the spinal cord but outside the cord itself. Meningiomas and nerve-sheath tumours such as schwannomas are the most common types of intradural extramedullary spinal tumour.
Causes of spinal cord tumours
The cause of tumours that start in the spinal cord or the membranes (meninges) covering the spinal cord is unknown. Research is being carried out into possible causes..
Signs and symptoms
These depend on the position of the tumour in the spinal cord. Spinal tumours often cause symptoms by pressing on the spinal nerves. Common symptoms include back and neck pain, numbness, and tingling and weakness in either the arms or legs or both.
Other symptoms can include clumsiness, and difficulty in walking. Tumours in the lower part of the spinal cord may cause loss of control of the bladder and bowel (incontinence).
Tests and investigations
In order for the doctors to plan your treatment they need to find out as much as possible about the type, position and size of the tumour. This is done by having a number of tests and investigations.
CT (computerised tomography) scan
This is a sophisticated type of x-ray, which builds up a three-dimensional picture of the inside of your spine. The scan is painless, but it will mean that you have to lie still for about 10-30 minutes. It may be used to find the exact site and size of the tumour, and identify the exact site of the tumour.
Before having the scan you may be given an injection of a substance to make the picture clearer. For a few minutes this may make you feel hot all over. It is important to tell your doctor and the person doing this test if you are allergic to iodine or have asthma before having the injection.
MRI (magnetic resonance imaging) scan
This test is similar to a CT scan, but uses a strong magnetic field instead of x-rays to build up cross-sectional pictures of your spine.
During the test you will be asked to lie very still on a couch inside a long tube for up to an hour. It is painless but can be slightly uncomfortable, and some people feel a bit claustrophobic during the scan. It is also noisy, but you will be given earplugs or headphones. You can usually take someone with you into the room to keep you company.
Before the test some people are given an injection of dye into a vein in the arm to improve the image, but this usually does not cause any discomfort.
The cylinder is a very powerful magnet, so before entering the room you should remove any metal belongings. People who have heart monitors, pacemakers or some types of surgical clips cannot have an MRI scan because of the strong magnetic field.
Treatment
The treatment for a spinal tumour depends on a number of things, including your age, general health, and the position, size and type of tumour. The results of your tests will enable your doctor to decide on the best form of treatment for you. There are some risks associated with treatment to the spine and your doctor will discuss these with you. The main treatments used are surgery, radiotherapy and steroids.
Surgery
The aim of the surgery is to remove the tumour without weakening the spine. Sometimes it is possible to remove spinal cord tumours completely, especially if the tumour is on the outer part of the spinal cord. If the tumour cannot be removed completely, it is often possible to remove part of it. This can help to slow down the progress of the cancer.
A surgical technique called a decompressive laminectomy is sometimes performed to relieve pressure within the spinal canal. Parts of several vertebrae are removed and also some of the tumour. This relieves pressure and can take tissue for a biopsy (to find out which type of tumour it is).
Radiotherapy
Radiotherapy treats cancer cells by using high-energy destroy the cancer cells while doing as little harm as possible to normal cells. It is usually given by directing radiotherapy rays at the tumour from outside the body – known as external radiotherapy. It is used to treat spinal tumours that have not been completely removed with surgery, or if the tumour comes back after initial treatment.
Steroids
Steroids are hormonal substances, naturally produced in the body by the reproductive organs and the adrenal glands above the kidney. Steroids can be given as tablets or by injection and can reduce the swelling that often surrounds spinal tumours. Although steroids do not treat the tumour itself, they are very useful in improving symptoms and making you feel better. They may be used before or after surgery, or before, during or after radiotherapy
Chemotherapy
The role of chemotherapy in the treatment of spinal tumours is still unclear. Research is being done to see whether chemotherapy is effective in treating these tumours.
Secondary spinal cord tumours
It is rare for a cancer elsewhere in the body to spread into the spinal cord but this may occasionally happen. The treatment used in this situation will depend on where in the body the primary cancer started.
Sometimes when a secondary cancer is affecting the spinal cord it can put pressure on the spinal cord and nerves, which can affect the function of the nerves. In this situation treatment needs to be given immediately, which usually includes radiotherapy and steroids (or occasionally surgery). The aim of the treatment is to shrink the tumour and to relieve pressure on the nerves. Once the pressure is relieved, further treatment may be needed and this depends on the site of the primary tumour that the secondary came from.
Clinical trials
New treatments for spinal cord tumours are being researched all the time, and you might be invited by your doctor to take part in a clinical trial to compare a new treatment against the best available standard treatment. Your doctor must discuss the treatment with you and have your informed consent before entering you into any clinical trial.
References
This section has been compiled using information from a number of reliable sources including:
- Oxford Textbook of Oncology (2nd edition). Souhami et al. Oxford University Press, 2002.
- Cancer and Its Management (4th edition). Souhami and Tobias. Oxford Blackwell Scientific Publications, 2003.
- Primary Tumours of the Brain and Spinal Cord (1st edition). Schold et al. Elsevier Science, 1996.
Page last modified: 02 November 2005
- Related information




